A REFERENCE COMPENDIUM
The WHI Study:
What the Headlines Got Wrong
How a misinterpreted 2002 study changed hormone therapy for a generation of women — and what the data actually shows

⚠️ NOT MEDICAL ADVICE
This compendium is for informational and educational purposes only. It is not intended to diagnose, treat, cure, or prevent any medical condition and should not replace guidance from a qualified healthcare provider. Always consult your doctor or a menopause specialist before making any decisions about hormone therapy or any other treatment.
⚡ FAST FACTS: KNOW THIS FIRST
The Women's Health Initiative (WHI) study published in 2002 caused a worldwide panic about hormone therapy
The "25% increased breast cancer risk" headline came from relative risk — not actual risk
The actual absolute risk increase was approximately 0.08% — or 1 extra case per 1,000 women per year
There was NO increased breast cancer risk during the first five years of treatment in any group
Estrogen-only therapy (tested separately) showed no increased breast cancer risk — and some data suggested a reduction
After 2002, HRT use dropped 40–80% worldwide — researchers later estimated this contributed to tens of thousands of preventable deaths
Modern menopause guidelines now support hormone therapy for many healthy women under 60 or within 10 years of menopause
What Was the WHI Study?
1991
The NIH begins recruiting for the Women's Health Initiative — one of the largest women's health studies in US history, costing $625 million.
1993–98
Over 160,000 postmenopausal women ages 50–79 are enrolled. The hormone therapy arm tests a specific drug combination against placebo. Notably, 67% of participants were between ages 60–79 — well past the typical age when women seek menopause treatment.
2002
The estrogen + progestin arm is stopped early. Results published in JAMA. Media headlines declare hormone therapy dangerous. Millions of women stop treatment. Many doctors stop prescribing it.
2003–07
HRT use drops by more than 46% in the US. In the UK, users fall from 2 million to under 1 million. No one is widely covering what this drop might be costing women.
2004–present
Hundreds of follow-up studies and reanalyses are published. Most conclude the original risks were overstated or misreported — but these receive a fraction of the media attention the original story did.
2025
The FDA convenes an expert panel to discuss the latest HRT evidence, with leading researchers calling for updated clinical guidance rooted in current science.
IMPORTANT CONTEXT
The WHI study was NOT designed to test whether hormone therapy is safe and effective for menopause symptoms like hot flashes and night sweats. It was designed to study long-term disease prevention in aging women. Those are very different research questions.
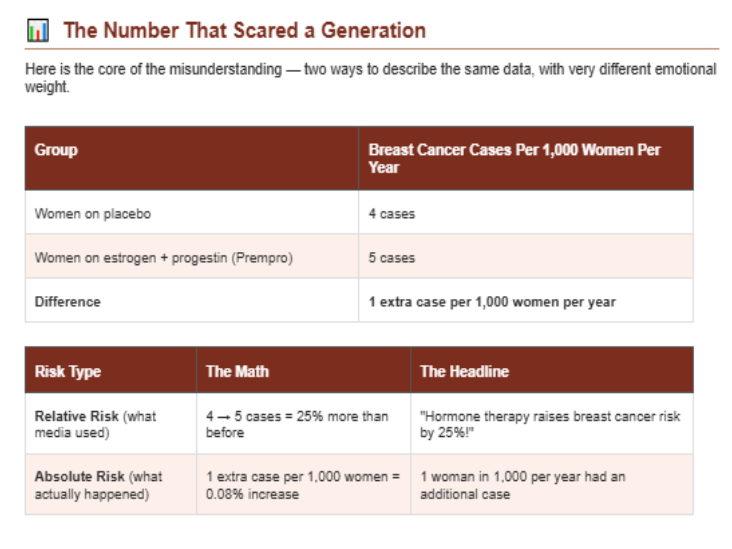
The Number That Scared a Generation
Here is the core of the misunderstanding — two ways to describe the same data, with very different emotional weight.
🧾 What Actually Happened
Women on placebo
4 cases per 1,000 women per year
Women on estrogen + progestin (Prempro)
5 cases per 1,000 women per year
Difference
1 extra case per 1,000 women per year
⚖️ Two Ways to Describe the Same Risk
📈 Relative Risk (what media used)
The math:
4 → 5 cases = 25% more than before
The headline:
“Hormone therapy raises breast cancer risk by 25%!”
📉 Absolute Risk (what actually happened)
The math:
1 extra case per 1,000 women = 0.08% increase
What that means:
1 woman in 1,000 per year had an additional case
WHY THIS MATTERS
Relative risk can make a tiny difference sound enormous. If a risk goes from 1-in-10,000 to 2-in-10,000, a headline can say "risk doubles!" — and still be mathematically accurate. That's the same trick that produced the 25% hormone therapy headline. In 2022, the Menopause Society officially stated that absolute risk is more appropriate for communicating hormone therapy information to patients.
0.08%
The actual absolute risk increase in the WHI data, Not the "25%" that made the news(Source: Estrogen Matters, Bluming & Tavris, 2018; The New Menopause, Haver)
FOR COMPARISON
Later analyses showed the increase in breast cancer risk from combined HRT was less than the risk associated with drinking alcohol regularly, smoking 10 cigarettes a day, or being obese. These comparisons rarely made the news.
6 Major Problems With the WHI Study Design and Reporting
FLAW 01
The Participants Were Too Old
The average WHI participant was 63 years old, often 10–20 years past menopause. Most women who seek hormone therapy do so in their late 40s or early 50s, near the onset of menopause. Results from a study of 63-year-olds cannot simply be applied to women who are newly menopausal.
FLAW 02
Only One Drug Combination Was Tested
WHI used Premarin (conjugated equine estrogen, derived from horse urine) combined with Provera (synthetic progestin), sold as Prempro. Today many women use bioidentical estradiol, micronized progesterone, or transdermal patches — none of which were studied in the WHI.
FLAW 03
Estrogen-Only Had the Opposite Result
The WHI had two separate arms: estrogen + progestin (for women with a uterus) and estrogen alone (for women post-hysterectomy). Media coverage lumped them together. Estrogen alone showed no increased breast cancer risk — and long-term follow-up suggested possible reductions in incidence and mortality.
FLAW 04
Many Participants Had No Symptoms
A significant portion of WHI participants had no hot flashes, night sweats, or menopause-related symptoms at all. Hormone therapy is typically prescribed for symptomatic women. Testing a treatment on people who don't need it raises serious questions about the relevance of the results.
FLAW 05
The Trial Was Stopped Early
The estrogen + progestin arm was halted before the full picture could emerge. Some of the WHI's own investigators later said they were not given enough time to review the final findings before publication — and that the results were too broadly interpreted from the outset.
FLAW 06
The Benefits Were Almost Entirely Ignored
Even in the original WHI data, hormone therapy was associated with reduced osteoporotic fractures, reduced colorectal cancer risk, and possible cardiovascular benefits for younger women. These findings received almost no media coverage.
The Timing Hypothesis: When You Start Changes Everything
One of the most important post-WHI discoveries is that the timing of hormone therapy — not just whether a woman takes it — appears to determine much of the risk-benefit picture.
SIMPLE ANALOGY
Studying hormone therapy in women who are 63 and decades past menopause, then applying those results to women who are 50 and newly menopausal, is a bit like studying the effects of exercise in 75-year-olds who've been sedentary for decades — then concluding that exercise is risky for everyone.
What current research shows:
A large Danish controlled trial (2012) found that women who began combined HRT immediately after menopause had a reduced risk of heart disease and death from heart disease over 10 years
A 2017 JAMA follow-up of WHI participants found hormone therapy was not associated with increased all-cause mortality over 18 years of follow-up
The North American Menopause Society, the Endocrine Society, and the British Menopause Society now all state that hormone therapy is appropriate for healthy symptomatic women under 60 or within 10 years of menopause
When Therapy Begins
Within 10 years of menopause, or before age 60
10–20+ years after menopause (like many WHI participants)
Potential cardiovascular protection, bone protection, symptom relief, possible reduced all-cause mortality
Different risk profile — existing arterial changes and years of vascular aging may affect how hormones interact with the body
💔 The Hidden Cost: What Happened After Women Stopped
After the 2002 headlines, millions of women stopped or never started hormone therapy. Years later, researchers began asking: what was the real cost of that fear?
18,000 – 91,000
Estimated premature deaths among women with hysterectomies who avoided estrogen therapy between 2002–2012, primarily from cardiovascular disease(Sarrel et al., American Journal of Public Health, 2013)
Why estrogen matters for more than hot flashes:
Estrogen supports healthy blood vessel function, cholesterol balance, and metabolic regulation
Heart disease is the #1 cause of death in women — it kills far more women than breast cancer
Estrogen also influences bone density, insulin sensitivity, and inflammation — all factors in long-term survival
Hip fractures in older women (often caused by low bone density) carry their own significant mortality risk
THE STATISTIC ALMOST NOBODY REPORTED
A 2017 follow-up study published in JAMA found that hormone therapy was NOT associated with increased all-cause mortality over 18 years. Women who started therapy earlier trended toward lower death rates in some analyses. This finding received almost no media coverage — because by 2017, the fear from 2002 had already become medical consensus.
Then vs. Now: How Understanding Has Shifted
What Updated Research Shows
The absolute risk increase was ~0.08% — less than the risk associated with obesity or regular alcohol use
Estrogen-only therapy showed no increased breast cancer risk; bioidentical and transdermal options were never studied
Age and timing of therapy dramatically change the risk-benefit picture; women under 60 starting near menopause have a very different profile
For symptomatic women under 60 or within 10 years of menopause, leading menopause societies now say benefits typically outweigh risks
When started early, HRT may reduce coronary disease risk and all-cause mortality in some groups
Even the original WHI data showed no increased breast cancer risk during the first five years of treatment — this was almost never reported
What 2002 Headlines Said
HRT increases breast cancer risk by 25%
All hormone therapy is the same
All women face the same risks from HRT
The risks outweigh the benefits
HRT increases heart risk
(Rarely mentioned) No elevated risk in first 5 years
Key Sources & Further Reading
Estrogen Matters (2018) — Dr. Avrum Bluming, M.D. & Dr. Carol Tavris — examines how WHI results were misrepresented and what the full data shows
The New Menopause — Dr. Mary Claire Haver — includes updated WHI analysis and current clinical guidance
Sarrel et al. (2013) — "The Mortality Toll of Estrogen Avoidance" — American Journal of Public Health
Cagnacci & Venier (2019) — "The Controversial History of Hormone Replacement Therapy" — PMC / NCBI
North American Menopause Society — menopause.org — current clinical guidelines
British Menopause Society & Women's Health Concern — current HRT guidance and history
WHI Original Publication — Writing Group for the WHI Investigators, JAMA, 2002
🗂️ THE SHORT VERSION
The 2002 WHI study tested one older synthetic drug on older, mostly symptom-free women — then reported results using statistics that made a tiny risk sound enormous
The "25% increased breast cancer risk" came from relative risk math; the actual absolute increase was less than 1 extra case per 1,000 women per year
Estrogen-only therapy showed no increased risk — and may have reduced it
There was no elevated cancer risk at all during the first five years of therapy in any group
The panic that followed may have contributed to tens of thousands of preventable deaths, mostly from cardiovascular disease
Today's guidelines support hormone therapy for healthy, symptomatic women under 60 — when the decision is based on truth, not a misread 23-year-old headline
Sources: Women's Health Initiative (JAMA, 2002); Sarrel et al., American Journal of Public Health (2013); Cagnacci & Venier, Medicina (2019); North American Menopause Society; British Menopause Society; Bluming & Tavris, Estrogen Matters (2018); Haver, The New Menopause. This document is for educational reference only and does not constitute medical advice.
Empowerment
Inspiring wellness tools for women’s health journeys.
Wellness
Healing
© 2025. All rights reserved.
Some pages on this site may contain affiliate links. If you purchase through these links, we may earn a small commission at no extra cost to you. We only recommend products we trust and believe provide value to our readers.